Article Text

Abstract
Objectives Across Canada, in the last decade, incidence rates of sexually transmitted and blood-borne infections (STBBI) have peaked (syphilis) or plateaued (hepatitis C virus (HCV) and HIV). Key populations (gay, bisexual and other men who have sex with men, trans and gender-diverse people, and people who use injection drugs) are at greater risk for these STBBIs, so correctly predicting risk before screening potentially infected individuals is crucial. We developed and validated a diagnostic clinical risk prediction model (CRPM) estimating HIV, HCV and syphilis risk for two key populations in two Canadian provinces.
Methods We used 20 variables and STBBI test results from a cross-sectional study evaluating multiplexed testing (detection of coinfections) in New Brunswick and Quebec (n=400) to develop our CRPM. We randomly split the data into development (n=300) and validation (n=100) datasets using clinic-stratified sampling. We used Bayesian predictive projection with development data to select ranked STBBI predictors. We obtained the ORs of the highest performing submodel measured as area under the receiver operating curve (AUC), sensitivity and specificity with 89% credible intervals (89% CrI) using validation data. Analyses were performed in R (≥V.4.2.3).
Results Out of 400 participants, 73 were infected with HIV (n=16), HCV (n=60), and/or syphilis (n=5). An internally validated submodel with two predictors (past drug injection, type of past sexually transmitted infection) displayed the highest AUC (0.79; 89% CrI 0.66 to 0.79), sensitivity (0.85; 89% CrI 0.79 to 0.91) and specificity (0.30; 89% CrI 0.15 to 0.50). The predictor contributing most to STBBI risk was past drug injection (OR=7.62; 89% CrI 4.41 to 13.07).
Conclusions This Bayesian-based CRPM is the first to identify high-risk individuals for HIV, HCV and syphilis with an overall good performance that minimises case missing. After additional validation, it could serve as a promising novel tool for prescreening key populations and improve Canadian STBBI multiplexed screening strategies.
- Risk Assessment
- HIV
- HEPATITIS C
- SYPHILIS
- Models, Statistical
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. To protect participants’ privacy, individual-level data are not available at this time. Descriptive statistics of all relevant variables before and after imputation are available as online supplemental material.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Clinical risk prediction models (CRPM) to identify individuals at higher risk of sexually transmitted and blood-borne infections (STBBI) have been developed and validated mostly for HIV and have shown variable performance.
In Canada, where STBBI incidence rates are currently rising or plateauing, only two frequentist statistics-based STBBI CRPMs have been developed to date, and neither targeted people who use injection drugs, gay, bisexual and other men who have sex with men, or trans and gender-diverse individuals of Quebec or New Brunswick.
WHAT THIS STUDY ADDS
To our knowledge, we have developed and validated the first data-driven Bayesian statistics-based hepatitis C virus (HCV), HIV and syphilis CRPM, which allowed us to obtain easily interpretable measures of uncertainty in the form of credible intervals (CrI).
The final model had good overall performance (area under the receiver operating curve=0.79; 89% CrI 0.66 to 0.79) that achieved a high sensitivity (0.85; 89% CrI 0.79 to 0.91), despite having low specificity (0.30; 89% CrI 0.15 to 0.50). If implemented, it would reduce the probability of erroneously identifying high-risk individuals as low-risk, which is key in STBBI screening programmes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We present a promising novel tool for prescreening individuals at high risk for HIV, syphilis and/or HCV that, after additional validation, has the potential to improve STBBI screening strategies if it is implemented in combination with targeted testing strategies in two distinct key populations.
Introduction
Context and rationale
In Canada, sexually transmitted and blood-borne infection (STBBI) incidence rates have either plateaued (eg, HIV, hepatitis C virus (HCV)) or increased (eg, syphilis) in the last decade, with an estimated 63 000 people currently living with HIV and 246 000 people with HCV.1 Syphilis, caused by Treponema pallidum, is experiencing an epidemic with 30 cases per 100 000, corresponding to a 178% increase over 10 years.1 Although survival attributed to treatment has improved, HIV was responsible for 104 deaths in 2018 and HCV case fatality rate was 7.4 per 100 000.1 2
Additionally, individuals belonging to key populations are at greater risk of contracting STBBIs because they are often stigmatised and discriminated against, including when accessing healthcare services.3 This situation increases their likelihood of healthcare avoidance, thus missing appropriate prevention, testing and treatment.3 Consequently, up to 14% and 44% of people infected with HIV and HCV, respectively, are unaware of their status.1 Gay, bisexual and other men who have sex with men (gbMSMs) accounted for 43.8% of new HIV cases in 2020 and 71% of all male syphilis cases in 2021.2 4 People who use injection drugs (PWID) accounted for 46.1% of HCV seroprevalence in 2019.1 No such data are available for trans and gender-diverse (TGD) individuals. In addition, coinfections, during which these pathogens interact in ways that influence disease susceptibility, progression and treatment outcomes, are common.1
Standard asymptomatic (ie, screening) and symptomatic testing strategies in Canada have not yet successfully reached these at-risk populations due to long turnaround time (TAT) and reliance on laboratory labour.5–8 Although point-of-care technologies designed to facilitate comfort with testing or decrease TAT by accurately detecting multiple infections simultaneously (eg, multiplexed testing) are being introduced into screening programmes, limitations based on linkage to care and reliance on confirmatory testing still remain.5–8 Calls to, improve, and deploy these technologies develop have specified that to amplify impact, models combined with these technologies would help target screening of those most at risk.1
Therefore, we used secondary data from a study evaluating a HIV, HCV and syphilis multiplexed screening strategy to develop and validate a diagnostic clinical risk prediction model (CRPM) for PWID, gbMSMs and TGD individuals from two distinct provinces.9 CRPMs are statistical tools that can be employed by physicians or patients to estimate the probability of a specific health outcome based on patient characteristics.10 Current STBBI screening strategies would benefit from diagnostic CRPMs used as prescreening tools to assist physicians in identifying those most at risk.11 Acceptable CPRM performance, corresponding to an area under the receiver operating curve (AUC; a combined measure of sensitivity and specificity) above 0.80, is crucial to minimise the number of high-risk individuals erroneously not encouraged to test (ie, false negative) and of low-risk individuals erroneously encouraged to do so (ie, false positive).11 Existing STBBI CRPMs have mostly focused on HIV prediction and shown variable performance (AUC: 0.49–0.89).11–13 CRPMs developed for other STBBIs (ie, CT/NG and HCV) showed variable performance (AUC: 0.49–0.99).14–16 The vast majority of existing CRPMs have used frequentist statistical development methods, but data-driven methods (ie, Bayesian statistics and machine learning (ML)) are increasing.16 17 Despite the predictive power of ML, its black-box nature often prevents intuitive result interpretation.18 We pursued a Bayesian framework that allows for a more intuitive interpretation of uncertainty through credible intervals (CrI).19 We previously developed a Bayesian-based HIV CRPM for individuals living in townships in South Africa (AUC: 0.71; 89% CrI 0.68 to 0.72).20 To our knowledge, only two STBBI CRPMs have been developed using Canadian data. Both employed frequentist methods, neither targeted key populations from these provinces, and only one was validated, highlighting limitations in CRPM data and methods.21 22
Objective
Therefore, we aimed to develop and validate a diagnostic prescreening CRPM that, if combined with multiplexed testing, could improve STBBI testing equity in Canadian key populations, especially PWID, gbMSMs and TGD individuals.
Methods
We followed the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (online supplemental tripod) statement (online supplemental checklist).10
Supplemental material
Data source
We recruited 401 participants from a cross-sectional study conducted at a community health clinic for gbMSMs and TGD individuals who have sex with men in Quebec (RÉZO; n=237) and a harm-reduction clinic for PWID in New Brunswick (RECAP; n=164), using convenience sampling.9 We evaluated an app-assisted multiplexed testing strategy through which we screened participants for HIV, HCV and syphilis using two immunological multiplexed tests and conducted confirmatory laboratory tests as per Canadian guidelines.23 We extracted all available deidentified variables in the app’s pretest questionnaire (predictors) and confirmatory test results (outcome). Predictors corresponded to relevant STBBI risk factors collected by nurses in the primary study. Details on inclusion/exclusion criteria, key study dates, sample size calculations, app interface and laboratory testing are reported elsewhere.9
Model specifications
We used participant self-reported categorical data as predictors without applying variable preselection for model development. We cross-checked testing history data with clinic records and when we found discrepancies, clinic records information was used. The outcome of interest was STBBI status (positive or negative). It was determined by positive confirmatory test results for HIV, HCV and/or syphilis (incident or existing acute or chronic infection) and negative confirmatory test results for all three. We identified new syphilis, HCV or HIV infections in participants testing positive who had no or unknown HIV, syphilis or HCV infection status history, excluding those that had spontaneously cleared or been treated for their HCV infections, when the information was available. Study staff were blinded to the outcome during predictor collection and laboratory staff were blinded to predictors and outcomes during confirmatory testing. All model metadata used in our analysis are described in table 1. Additional variable handling details are in online supplemental methods and sensitivity analysis.
Supplemental material
Clinical risk prediction model metadata by variable category
Missing data
We imputed 446 missing data from 77 individuals using multiple imputation by chained equation (MICE) implemented within the mice package.24 We found no missing data for STBBI status. We excluded one individual from model development due to >50% missing data. Missing data pattern for some variables depended on clinic (online supplemental figure S1). Thus, we included clinic location as a dummy variable and imputed data with the appropriate Bayesian regression (table 1).24 We imputed data in five datasets, evaluated its validity and pooled values for the remainder of the analysis (online supplemental figure S2 and online supplemental methods and sensitivity analysis).
Supplemental material
Supplemental material
Predictive projection
With the pooled imputed datasets, we conducted variable selection by predictive projection (ie, projection of the posterior of the full model onto each candidate submodel), a robust method for high-dimensional datasets (ie, relatively small sample sizes compared with the number of variables).25 We separated our data into development (ie, training; n=300) and validation (ie, testing; n=100) datasets using clinic-stratified random sampling to ensure representation of both sites in each set. We fit then development data with a full Bayesian logistic regression reference model containing all predictors (ρ=20) and STBBI status as the outcome variable.25 By including clinic location in the full model, we adjusted it to account for differences and confounding in each key population. We assigned horseshoe priors (τ=0.02) for all coefficients.25 We then selected the sparsest submodel with a performance equivalent to the full model and reduced the CRPM complexity (online supplemental methods and sensitivity analysis).
Model evaluation
We evaluated the predictive accuracy of nine submodels with performances (ie, estimated log predictive density (ELPD)) closest to the full model using a method independent from accuracy value thresholding. We computed sensitivity and specificity from 2000 draws of submodels posterior predictive distribution for STBBI status and AUC from expected values of these draws. We quantified uncertainty using 89% CrIs to increase stability with effective sample sizes below 10 000 and to avoid confusion with 95% CIs.26 We selected the final model with the best AUC obtained with the validation dataset. We then computed the OR and associated 89% and 95% CrIs from each coefficient in the final fitted model to inform the contribution of each predictor.
All analyses were done in R (≥V.4.2.3).27
Sensitivity analysis
In a sensitivity analysis, we examined differences in behaviour between incident and existing STBBI cases and compared results obtained with imputed data to those obtained with complete case data (n=323). We also compared the final CRPM with CRPMs developed with HIV/syphilis, HIV/HCV and HCV as outcomes (online supplemental methods and sensitivity analysis).
Results
Participant recruitment and characteristics
In the original study, we recruited 400 participants from RÉZO (nn=236) and RECAP (nn=165), excluding the removed individual. Most participants (63.75%) self-identified as male, with 18.25% as female and 1.75% as transgender. Nearly half of all participants (49.25%) were 35 years old and above. We identified 73 STBBIs, corresponding to 16 HIV, 5 syphilis and 60 HCV infections. Of these, eight were coinfections (five HCV/HIV and three HIV/syphilis) and 20 were new infections. Additional details about visit procedures, multiplexed test results and treatments are described elsewhere.9
Due to key population differences in density, risk factors and needs, RECAP had a greater HCV infection proportion (78.33%) while RÉZO had greater HIV (100%) and syphilis (80%) infection proportions. RECAP also had a greater proportion of individuals reporting using injection drugs in the past (29.75%) than RÉZO (5.5%). We also observed differences in gender, descent, education, income and work status by clinic. The distribution of each characteristic by clinic is outlined in online supplementary table S2 for each dataset.
The outcome (ie, STBBI status) was similarly distributed between the development (17% positive cases) and validation datasets (20% positive cases). The distributions of variables in the pooled imputed datasets (m=5) are shown in online supplemental table S2.
The submodels reached the predictive performance of the full model with nine ranked variables
To develop a simple CRPM with a reduced number of predictors of STBBI infection, a sample size of 300 was sufficient to use predictive projection feature selection on a full model with all predictors (ρ=20).25 We found that most of the full model predictor’s posteriors had CrIs spanning the null due to horseshoe prior effects (online supplemental figure S3).
Supplemental material
Based on predictor ranking agreement between cross-validation folds (online supplemental figure S4), we identified the nine sparsest submodels with ELPD closest to the reference model. As expected, when we fitted each submodel with the development dataset, the AUC increased as the number of predictors increased, until reaching the value of the full model (AUC=0.84; 89% CrI 0.8 to 0.86) (figure 1). Submodels 2 to 9 had an acceptable AUC (>0.80). Sensitivity remained very similar, between 0.85 (89% CrI 0.81 to 0.43) and 0.87 (89% CrI 0.83 to 0.91), and so did specificity, between 0.32 (89% CrI 0.21 to 0.43) and 0.38 (89% CrI 0.26 to 0.49), across all submodels (online supplemental figure S5).
Supplemental material
Supplemental material

Area under the receiving operating characteristic curve (AUC) of nine submodels and the full reference model (p = 20) fitted with the development (blue; n = 300) and validation (purple; n = 100) datasets. We measured AUC based on the values of expected STBBI status based on 2000 samples drawn from the posterior predictive distributions. On the x-axis, each predictor named represents the submodel containing it and all predictors to its left. The reference model contains all available predictors. The AUC of the submodels fitted with the development (ie, training) dataset increased by submodel size whereas the submodel containing two predictors had the highest performance when fitted with the validation (ie, testing) dataset. Each point represents the median and each line represents 89% credible intervals of the variation in expected STBBI status values obtained from each predictor present in each model. STBBI, sexually transmitted and blood-borne infections.
The submodel with two predictors had the best performance with the validation dataset
When we fit these submodels with the validation dataset (n=100) (table 1), we found that the submodel with past drug injection and type of past STI test had the best performance with an AUC of 0.79 (89% CrI 0.66 to 0.79), a sensitivity of 0.85 (89% CrI 0.79 to 0.91) and a specificity of 0.30 (89% CrI 0.15 to 0.50) (online supplemental figures 1 and 5). All other submodels had AUC values of 0.72 (89% CrI 0.70 to 0.45) to 0.78 (89% CrI 0.72 to 0.82) and similar values for sensitivity, between 0.85 (89% CrI 0.79 to 0.45) and 0.86 (89% CrI 0.79 to 0.91) and specificity, between 0.30 (89% CrI 0.10 to 0.45) and 0.35 (89% CrI 0.20 to 0.50).
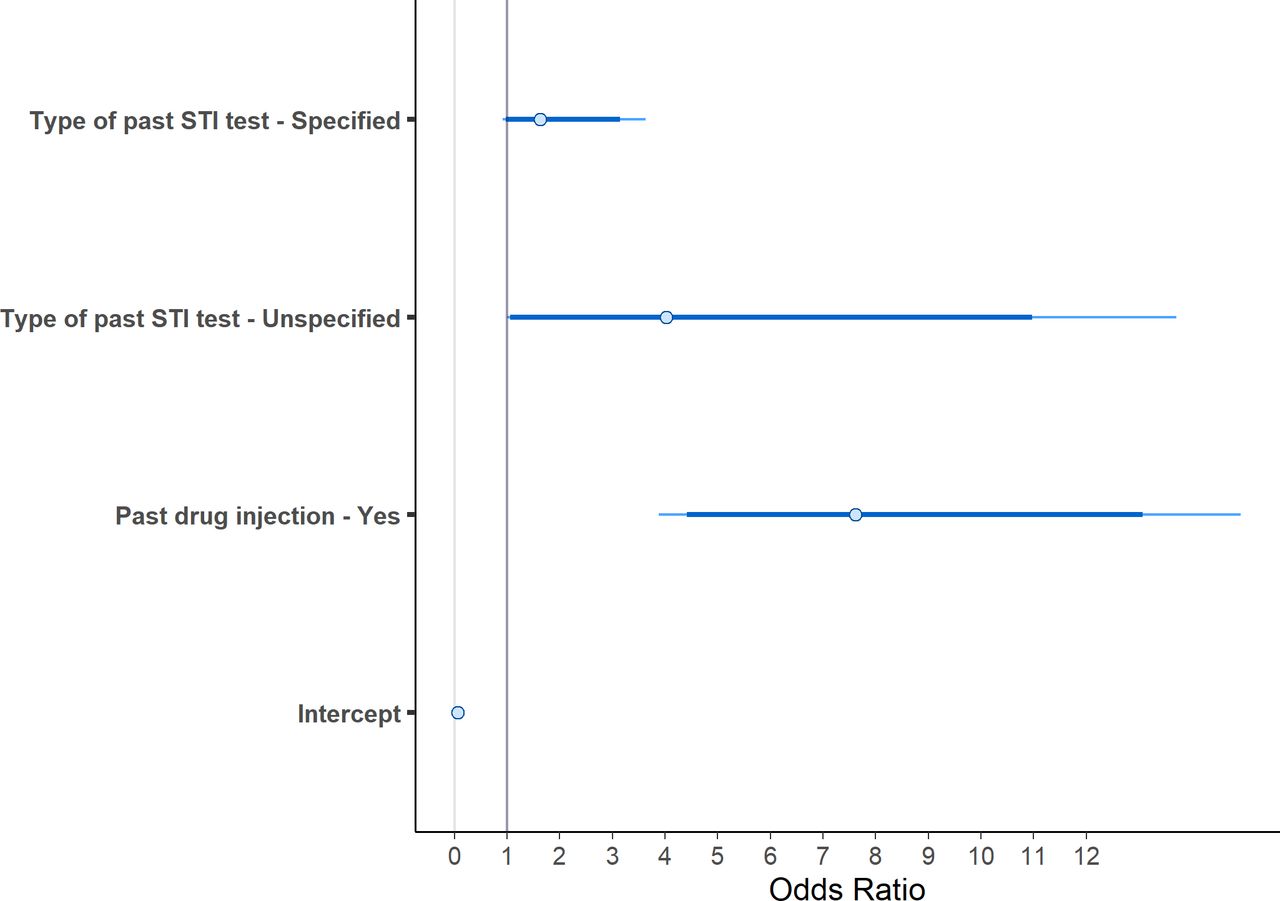
The predictor with the strongest effect on STBBI risk (ie, indicating a positive diagnosis) was past drug injection (OR=7.62; 89% CrI: 4.41 to 13.07) (figure 2).

{kind=link}
{kind=link}
Median, 89% (thick segment) and 95% credible intervals (thin segment) of estimated OR for the intercept and each predictor of STBBI status in the final submodel (p=2) fitted with the validation (ie, testing) set (n=100) based on 2000 draws of the predictive distribution. The vertical line represents null effect (OR=1.0). STBBI, sexually transmitted and blood-borne infections.
Sensitivity analysis
We found little to no difference in behavioural variables’ distributions between incident and existing STBBI cases (online supplemental table S3), which the imputation was successful, and some differences in prediction depending on STBBI of interest (online supplementary methods and sensitivity analysis).
Using the final model
To use the final model, physicians should input patient past drug injection (ie, yes or no) and type of past STI test (ie, specified, unspecified or none) information. The CRPM will then output a risk probability, and they can decide whether to offer testing (table 2).
Risk of sexually transmitted or blood-borne infection (STBBI) by predictor in the final model (p=2)
Discussion
Interpretation
Overall, the results obtained with the validation dataset had a slightly lower performance and greater uncertainty than those obtained with the development dataset. A final CRPM with a nearly acceptable AUC (ie, 0.79) is encouraging considering its intended use as a prescreening tool to identify high-risk individuals and offer them testing.11 We obtained higher AUC measures than with a HIV CRPM that we previously developed using South African data, although greater uncertainty due to smaller sample size.20 In addition, these validation values are on the higher end of existing STBBI CRPMs and include uncertainty measures which are often lacking.11–13 16 17 In addition, unlike with most existing ML models, sensitivity was always higher than specificity, resulting in fewer false positives than false negatives.16
PWID are known to be at higher HCV risk.1 Thus, due to numerous HCV-positive cases in our dataset (n=60), a CRPM with past drug injection as the most important predictor performed as expected. It was also identified as an important predictor of STI risk in another existing Canadian CPRMs, but its predicting ability was not quantified.21 Predictor ranking only differed when we removed HCV cases, which may indicate that the final CRPM will perform better with an HCV-infected individual.
Strengths and limitations
To our knowledge, we developed and validated the first Bayesian HCV, HIV and syphilis CRPM. Using this approach allowed us to incorporate sparsity assumptions into our model with horseshoe priors and to output easily interpretable uncertainty probability measures (ie, CrIs).19 Using predictive projection, we obtained a simple model containing two predictors, which will be useful in rapidly identifying high-risk individuals who would benefit from STBBI testing. Unlike other previously developed CRPMs, we validated our CRPM internally using cross-validation with the development dataset and through random splitting of our initial dataset.10–14 16 In addition, the performance of candidate submodels based on draws of the posterior distribution allowed us to use a threshold-independent calculation of the sensitivity, specificity and AUC. Threshold-based measures are often assigned arbitrarily and decided based on very specific clinical context that can impact generalisability.28
Although a single joint model that predicts risk in two key populations with overlapping risk factors and infections has merit, the limited data source size obtained from two heterogeneous populations could have impacted its validity. To address the small sample size, we employed a method that generates robust models from scarce datasets.25 To address the heterogeneity, we considered developing a separate model for each population. However, the limited sample size and numerous missing data in the RECAP dataset prevented this, because MICE is not robust with high proportion of missing values. Instead, we accounted for key population differences with the clinic location variable in each step of our analysis, including in the reference model, where it accounts for the interpopulation heterogeneity. Grouping incident and existing cases as positive cases may have led to confounding bias from difference in behaviours between those with and without awareness of their status. However, the distribution of most behavioural variables did not differ between these groups. In practice, a low-specificity CRPM could lead to labour, psychological and monetary costs associated with low-risk individuals encouraged to test.29 However, low specificity is preferable to low sensitivity by minimising the number of missed high-risk individuals for targeted testing.29 By sourcing data from a cross-sectional primary study using convenience sampling, conducted in urban centres, any bias resulting from the selection of participants that frequently visit these clinics may have impacted the generalisability of our results.9 Despite using rigorous imputation methods, we are not guaranteed that missing data followed the same pattern as observed data. Additionally, residual confounding may have been introduced when grouping variables and from uncollected variables (eg, partner STBBI status). The absence of methods to incorporate coinfection mechanisms in our final model may limit its predictive accuracy for coinfected individuals. We could consider a multivariable regression to jointly model the correlated risks of coinfections in the future. Finally, apart from testing history, for which clinic records were available, app-based predictor data were self-reported from an interview with a nurse, which may have been impacted by social desirability bias. However, in practice, CRPM users will have to declare their information to the healthcare provider to receive their risk probability.
Implications
Our results are aligned with Canadian elimination targets for three STBBIs and calls to improve current screening strategies.1 By providing a validated CRPM specific to two key populations in two Canadian provinces, with acceptable performance, we are providing decision-makers with a novel prescreening tool that can be used in combination with targeted testing strategies to improve multiplexed testing initiatives for these populations. Currently, any individual belonging to a key population is encouraged to test frequently, with less emphasis on individual risk, and the monetary and time cost of all administered tests constitute major deterrents to upscaling these initiatives. A simple CRPM that can identify those at truly greater HIV, HCV and/or syphilis risk within those populations while minimising case missing can assist healthcare providers in offering screening on an individual basis and decrease overall testing costs.
In the future, we plan to conduct additional validation and updating in other global populations that would benefit from targeted STBBI screening (eg, rural populations in India), which we will source from larger homogenous study populations using a sampling method less prone to bias, with incident cases, more syphilis cases, and including mechanisms of coinfections, to confirm our model’s performance in key populations and improve on the current limitations of our CRPM.
In addition, costs required for successful implementation and maintenance of a CRPM do not guarantee an improved cost-effectiveness compared with current screening strategies.30 Thus, our CRPM would benefit from a cost-effectiveness analysis.
Finally, assigning risk to an individual can be stigmatising and depends on the CRPM user’s willingness to share their information with healthcare providers. Therefore, our CRPM should be evaluated by members of the targeted community to ensure use of inclusive and appropriate language before implementation.
In conclusion, we have developed and validated a promising tool to prescreen individuals at high risk for three STBBIs with the potential to improve screening strategies. After additional validation and evaluation, the CRPM could identify and encourage high-risk individuals to use multiplexed screening interventions for HCV and related coinfections.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. To protect participants’ privacy, individual-level data are not available at this time. Descriptive statistics of all relevant variables before and after imputation are available as online supplemental material.
Ethics statements
Patient consent for publication
Ethics approval
We obtained ethics approvals from the Research Institute of the McGill University Health Centre (protocol number: 2020-6048) and from the Horizon Health Network Research Ethics Board at the Saint John Regional Hospital (protocol number: 2020-2963)
Acknowledgments
The authors would like to thank Melisa Eraslan and Juhi Tulsi for their help with the manuscript uploading process and Cindy Leung Soo for her guidance on coding for risk prediction modeling. The authors also extend their gratitude to the participants of the AideSmart! study, who donated their time and information and the study staff, for meticulously collecting this data.
References
Footnotes
Handling editor Jamie Scott Frankis
Contributors NPP conceived and designed the project. Data were obtained from a cross-sectional study evaluating multiplexed testing in Canada. DW, SM and ADB were responsible for participant recruitment and data collection. FV cleaned, prepared and imputed the data with guidance from QZ and NPP. FV developed and validated the reference model and submodels with guidance from QZ. QZ verified the codes and data. NPP, QZ, SB and SN contributed to results and provided extensive feedback to contextualise findings. FV wrote the first manuscript draft, and all authors read and approved the final manuscript. NPP is responsible for the overall content as the guarantor. Non-author contributors: AK led the implementation, analysis and publication of the primary study. Cindy Leung Soo developed the first version of the code for Bayesian risk prediction modelling, from which FV based themselves to develop the code in this analysis. ME and JT provided support during the manuscript uploading process.
Funding This study was funded by the Canadian Institutes of Health Research (grant PJT153149). The study sponsor had no role in study design, collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication. NPP acknowledges support from the Fonds de recherche du Québec - Santé (Senior Scientist award 252845, Distinguished Research Scholar award 324154) and the India-Canada Centre for Innovative Multidisciplinary Partnerships to Accelerate Community Transformation and Sustainability (IC-IMPACTS; CNO 3072). FV is funded by a Fonds de recherche du Québec - Santé Master’s Training scholarship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.