Article Text

Abstract
Objectives There is limited evidence about the prevalence of oropharyngeal gonorrhoea (OPNG) in heterosexuals. To test the hypothesis that the oropharynx acts as a reservoir for gonorrhoea, potentially contributing to high rates of infection, we assessed OPNG positivity in self-sampling individuals.
Methods From November 2023 to March 2024, SH:24, an online postal self-sampling service, expanded gonorrhoea (NG) nucleic acid amplification testing to include oropharyngeal swabs for heterosexual individuals aged 17–24 years in Northern Ireland and Ireland. Participants were included if they identified as heterosexual with no same or both-gender sexual partners. Positivity was compared by sex and infection site, with χ2 tests. Island-of-Ireland weighted positivity with 95% CI was estimated.
Results OPNG was detected in 92% (208/226) of NG cases, representing 2.9% (95% CI 2.6 to 3.4) of the tested population. Single-site OPNG infections accounted for 63% (143/226) of cases, corresponding to an overall single-site oropharyngeal positivity of 1.9% (95% CI 1.7 to 2.4). Genital-only infections occurred in 8% (18/226) of cases, while concurrent oral and genital (multisite) infections were identified in 29% (65/226). Overall NG positivity (across all anatomical sites) was 3.2% (226/7009; 95% CI 2.8 to 3.7). Of 12 011 individuals who requested a self-sampling kit, 7036 (58.6%) returned both oropharyngeal and genital swabs suitable for analysis, with valid test results available for 7009 individuals.
Conclusions Our findings suggest the oropharynx is a common NG infection site among young heterosexuals, often occurring independently of genital infection. Most OPNG cases (63%) did not coincide with genital infection and would have been missed by testing protocols limited to urogenital sites. These results suggest a potential risk for onward transmission, the need to consider a review of testing guidelines in this population and further research to better understand behavioural risk factors associated with OPNG positivity.
- gonorrhea
- Neisseria gonorrhoeae
- prevalence
- communicable diseases
- population surveillance
Data availability statement
No data are available. All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is a lack of estimates of oropharyngeal gonorrhoea in young heterosexuals, despite recognised transmission risks and potential public health implications.
Existing literature has primarily focused on populations considered to be at high risk, such as female sex workers, gay, bisexual and other men who have sex with men and heterosexual cisgender men and women with a known exposure to gonorrhoea.
The hypothesis that the oropharynx may serve as a reservoir contributing to ongoing transmission in the broader population has not been adequately studied, necessitating this research to better understand its role in young heterosexuals.
WHAT THIS STUDY ADDS
By widening home-based, self-sampled online sexually transmitted infection (STI) testing across the island of Ireland to include an oropharyngeal swab for young people self-reporting as heterosexual, we have assessed community-based oropharyngeal gonorrhoea positivity in this population.
This approach provides new insights into the presence of oropharyngeal infections, including cases that occurred without concurrent genital infection, among mainly asymptomatic individuals.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Offering additional testing for oropharyngeal gonorrhoea resulted in a substantial increase in gonorrhoea case acquisition beyond existing genital cases in a real-world setting.
These findings suggest that incorporating oropharyngeal gonorrhoea sampling into routine STI testing for young heterosexuals would identify cases currently missed by genital-only testing.
While routine universal testing would be the most effective way to detect the majority of infections, further research is needed to better understand the transmission dynamics and behavioural factors associated with oropharyngeal gonorrhoea in individuals who do not identify as men who have sex with men and to evaluate the cost-effectiveness of routine oropharyngeal gonorrhoea testing
Introduction
Notifications of Neisseria gonorrhoeae have increased across European Union/European Economic Area countries with diagnoses rising by 59% between 2018 and 2022. Young heterosexual people are increasingly being recognised as a risk group, with the highest age-specific rates observed among those aged 20–24 years; 99.6 cases per 100 000 in men and 48.1 cases per 100 000 in women. Although gay, bisexual and other men who have sex with men (GBMSM) continue to account for the largest number of gonorrhoea diagnoses, heterosexuals have experienced a greater proportional increase. Between 2021 and 2022, gonorrhoea incidence among heterosexuals rose by 50% overall, compared with a 30% increase among GBMSM during the same period.1 This trend is also evident on the island of Ireland (IOI: both Northern Ireland (NI) and Ireland). Between 2019 and 2022, NI reported an 86% increase in gonorrhoea diagnoses, with heterosexual males and females experiencing rises of 81% and 96%, respectively.2 Similarly, Ireland saw increases in case numbers for those aged 15–24 years in both males and females, 54% and 57%, respectively.3
The underlying reasons for the increase in heterosexual gonorrhoea diagnoses are not fully understood. Hypotheses include changes in sexual behaviours,4 such as increased rates of partner change5 and increased interconnectedness of sexual networks,6 as well as the role of bridging populations, such as men who have sex with both men and women.7 Additional proposed factors include increased access to STI testing and greater transmissibility of NG strains that cause fewer symptoms within heterosexual networks.1 8
At the time of writing, guidelines from the British Association for Sexual Health and HIV (BASHH) and the Health Service Executive (HSE) recommend routine rectal and pharyngeal testing for NG in GBMSM. However, oropharyngeal testing in heterosexuals is advised only under specific circumstances, such as in sexual partners of confirmed cases or where ceftriaxone resistance is detected from a genital isolate. This selective testing strategy has resulted in a knowledge gap regarding the prevalence of oropharyngeal N. gonorrhoeae (OPNG) in heterosexual populations.9 10
In response to national and European trends showing a rise in NG diagnoses, a pilot expansion of testing policy was implemented across IOI. This involved widening the test offer for OPNG through SH:24 to heterosexuals aged 17–25 years. SH:24 is the provider of an online postal self-sampling service (OPSS) for STIs, funded as a public health service and available to individuals aged 16 years and over in NI and 17 years and over in Ireland. SH:24 service provides free home sampling kits that are returned to a centralised laboratory for testing. Both symptomatic and asymptomatic users were able to request and receive postal self-sampling kits. This expansion applied to the OPSS only and did not alter in-clinic testing protocols.
This coordinated approach facilitated universal community-based OPNG testing among young heterosexuals accessing OPSS, enabling assessment of OPNG positivity within this population.
Methods
Objectives
We aimed to investigate the positivity of oropharyngeal gonorrhoea among young heterosexual people on IOI, by offering universal OPNG testing through the SH24 online STI sampling service from November 2023 to March 2024.
Study population
Individuals aged 17–25 years who ordered and returned a home STI sampling kit via the free online service provided on the IOI were eligible for inclusion. Participants who met the following criteria were included in the analysis:
Inclusion criteria
Aged 17–25 years on the day of kit request.
Self-identified as heterosexual.
Resided on the IOI.
Exclusion criteria
Gender identity combined with “Who do you have sex with?” response indicated same-gender contact.
Response to “How would you describe your sexual orientation?” was one of: gay man, lesbian, bisexual, in another way or prefer not to say.
Additional information
A unique identifier was assigned to each service user, preventing repeat test orders within a 3-month period; data validation confirmed that no repeat tests were included in the analysis.
Study procedures
Between November 2023 and March 2024, the established home sampling process for STIs was expanded to include an oropharyngeal swab for eligible participants. The standard sampling kit comprised either a vulvovaginal swab or a urine sample collection vessel, based on the individual’s genitals for combined chlamydia/gonorrhoea testing. In addition to these, during the study period, all participants received an oropharyngeal swab specifically for gonorrhoea testing. Users of the service were informed at the time of ordering that their STI testing kit included this oropharyngeal test. Participants were required to return their samples in a freepost box, sealed with a tamper-evident seal sticker. Cases of oropharyngeal or genital gonorrhoea were referred to sexual health services for management and treatment in line with BASHH/HSE guidelines, as is usual practice.
Data collection
At the time of ordering an OPSS, participants answered a set of routine questions including sociodemographic information and questions about their reasons for seeking a test, sexuality and sexual preferences. This is a standard part of requesting any STI testing kit from the OPSS. No new questions were added. Data were systematically collected via the SH:24 online portal. SH:24 managed handling and storage procedures for all participant data in compliance with the General Data Protection Regulation and Data Protection Act (2018).
Laboratory testing
Urogenital gonorrhoea testing was performed on first-void urine specimens in men and vulvovaginal swabs in women. Nucleic acid amplification tests (NAATs) were used to detect N. gonorrhoeae (and Chlamydia trachomatis) in all specimens, using the Aptima Combo2 assay (Hologic). Positive results for NG were confirmed using the single analyte Aptima GC assay. To control for possible underestimation of positivity or skewed anatomical site distribution, we limited analysis to data from patients with a valid test (positive or negative) from both anatomical sites.
Data analysis
All analyses were conducted using R software, V.4.2.1. Participants were grouped into several (not mutually exclusive) NG categories: NG positive, NG negative, OPNG positive and genital positive. NG positive cases were further stratified into exclusive subcategories: OPNG multisite, OPNG only and genital NG only (table 1). Quantitative variables, such as age, were analysed for measures of central tendency. Frequencies and percentages were calculated for categorical variables. The terms ‘men’ and ‘women’ refer to cisgender men and cisgender women, respectively, and hereafter will be referred to as women and men for brevity. For the calculation of individual positivity rates for NI and Ireland, no weighting was applied; however, the overall IOI combined positivity was weighted to account for differences in sample size, with 95% CIs calculated using the binomial exact method. Categories for reporting NG positivity were selected based on sample size adequacy to ensure estimates had sufficient statistical power. ORs were calculated to assess the strength of associations. Pearson’s χ2 test was applied to evaluate associations between demographic categories and OPNG positivity, and the Kruskal-Wallis rank sum test was used to assess age differences. A p value of <0.05 (two-tailed) was considered statistically significant. Unless otherwise stated, missing or ‘other’ responses accounted for slight variations in sample size, with missing data not imputed.
Definitions of Neisseria gonorrhoea test result categories
Results
Study population characteristics
A total of 12 011 home STI sampling kits were dispatched to the study population on IOI during the study period. Of these, 7036 kits were returned, representing an overall return rate of 58.6%. A higher proportion of kits were returned in NI than in Ireland (1277/1907, 67% vs 5759/10 104, 57%; p<0.001). When comparing sex, ethnicity and the reason for seeking a test, there were no significant differences between those who returned the kit and those who did not (p>0.05). Among the returned kits, 7009 yielded valid laboratory results for both genital and oropharyngeal specimens (n=27 excluded). Among these individuals, most identified as White ethnicity (96%), had a median age of 22 years (IQR 20–24) and three-quarters were female (n=5290) participants. Regarding the reasons for testing, one-third reported experiencing symptoms associated with an STI (n=2243), while the majority underwent asymptomatic testing (n=4696).
Neisseria gonorrhoeae positivity
No significant differences in overall NG positivity or in the distribution of infection sites were detected between NI and Ireland (p>0.05). Consequently, results were pooled and presented for IOI. Of the 7009 individuals tested on IOI, 3.17% (226/7009; 95% CI 2.82 to 3.67%) were positive for gonorrhoea. Among these cases, 92% (208/226) had OPNG, equating to an overall OPNG positivity of 2.87% (95% CI 2.58 to 3.39%). Genital infection was observed in 36% (83/226) of the positive cases, corresponding to an overall genital positivity of 1.18% (95% CI 0.94% to 1.47%). Within the genital infections, 18 were genital-only (0.31%, 95% CI 0.15% to 0.41%), while 65 had concurrent genital and oropharyngeal infections (0.94%, 95% CI 0.72% to 1.18%). OPNG-only infections comprised the majority of cases, accounting for 63% (143/226) with an overall positivity of 1.92% (95% CI 1.72% to 2.40%) (table 2).
NG test results by infection site
Characteristics of participants by Neisseria gonorrhoeae category
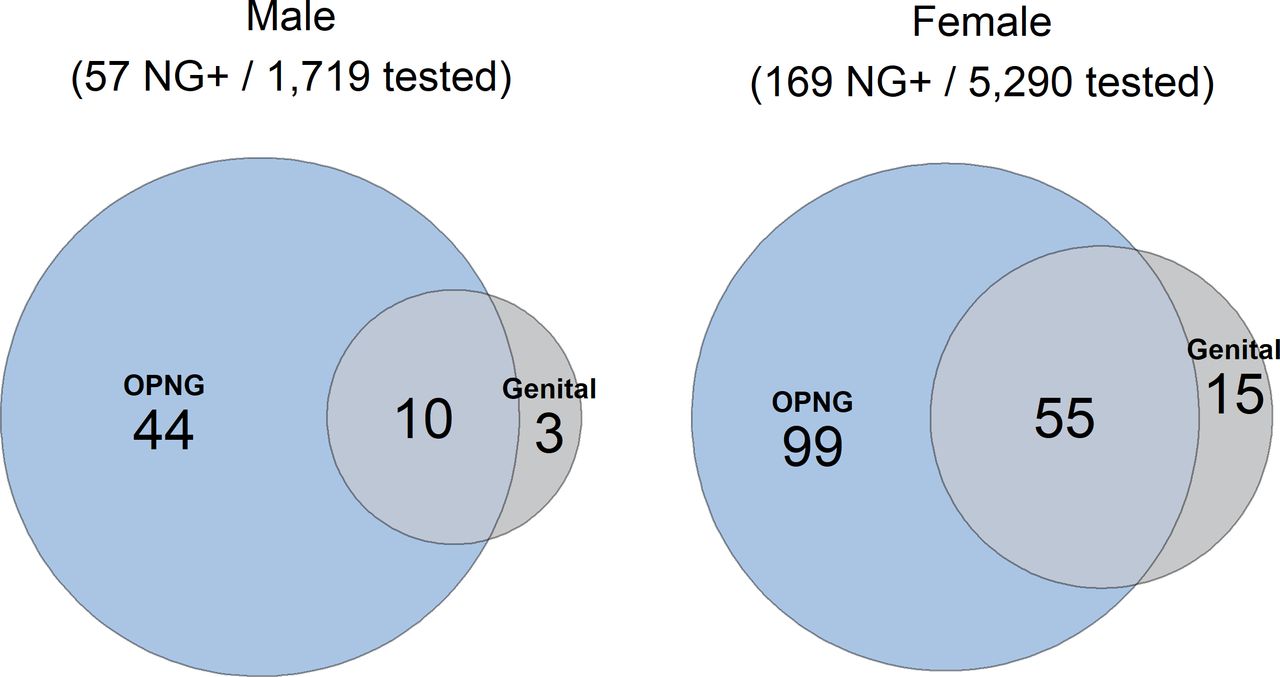
Among all NG cases, 69% (156/226) were asymptomatic at the time of testing, while 31% (70/226) reported experiencing genital symptoms consistent with an STI. Among individuals in exclusive NG categories: genital NG only (n=18), OPNG only (n=143) and OPNG multisite (n=65), no significant differences in age distribution were observed (Kruskal-Wallis rank sum test, p>0.05). Positive NG test results by anatomical site among NG cases are shown as a Venn diagram in figure 1. Overall NG positivity was similar between males (3.32%, 57/1719) and females (3.19%, 169/5290); however, a significantly higher proportion of NG-positive males had OPNG-only infections (77.2%, 44/57) compared with females (58.6%, 99/169; p=0.01). No significant differences were observed in the proportions of genital-only infections (males: 5.3%, 3/57 vs females: 8.9%, 15/169; p=0.62) or oral multisite infections (males: 17.5%, 10/57 vs females: 32.5%, 55/169; p=0.11).

{kind=link}
Distribution of Neisseria gonorrhoeae (NG) infections by anatomical site.
Discussion
This study is set within the context of a doubling in gonorrhoea diagnoses in young people (aged 15–24 years) from 2013 to 2022.8 The overall positivity for NG among young heterosexuals undergoing home sampling for STIs on IOI was 3.17%. OPNG was more common than genital gonorrhoea, with a positivity rate of 2.87% compared with 1.18% for genital infections (p<0.01). Among individuals who tested positive for NG, 92% had oropharyngeal infection, with 63% having infection confined exclusively to the oropharynx, representing cases that would have been missed by current genital-only testing protocols. In terms of STI symptoms, many cases were asymptomatic, consistent with existing literature.11 These asymptomatic individuals would not have been offered OPNG testing unless specific conditions were met, such as being identified through partner tracing or meeting defined risk criteria.
While surveillance efforts for OPNG have primarily focused on traditionally higher-risk populations, such as GBMSM12–14 and female sex workers,15 16 emerging evidence suggests that OPNG is not uncommon among heterosexual individuals.9 17–20 To our knowledge, our investigation is the first to estimate OPNG prevalence in a non-selected heterosexual population by expanding an online STI sampling service to include users in a community setting. OPNG positivity among women was 1.87%, with 58% of female NG cases being OPNG-only. These findings are consistent with previous reports in female sexual health clinic populations, where OPNG prevalence has ranged from 1.4% to 2.8%, with 48%–55% of cases being OPNG-only.15 21 These findings presented here also align with the limited studies that have included heterosexual men. Chow et al 18 found that among heterosexual individuals reporting sexual contact with partners with gonorrhoea, 89% of NG cases in men and 40% in women were confined to the oropharynx. Similarly, this analysis found OPNG-only cases to be more frequent in men (77.2%, 44/57) than in women (58.6%, 99/169).
A limitation of this study is the lack of behavioural data, which restricts our ability to assess specific risk factors and associations for OPNG. For example, the number of recent sexual partners and sexual practices, such as oral sex or kissing, was not captured in the routine pretesting questionnaire. Studies in GBMSM have identified oral sex as a key mode of NG transmission, with the oropharynx acting as a reservoir for untreated and asymptomatic infections.22 Similarly, among female NG contacts, those testing positive at the pharynx are more likely to report giving oral sex than those testing negative for OPNG.23 Additionally, evidence indicates that OPNG can be transmitted through condomless oral sex and through non-coital activities such as kissing.24–27 The absence of such data in our study restricts our ability to confirm these associations within the IOI population.
The population of heterosexuals proactively seeking home STI sampling is not expected to be representative of young heterosexuals in the general population. The service provided, and consequently our study, relies on self-reported sexuality and sexual behaviours for inclusion. This introduces potential bias, as some individuals may prefer not to disclose their sexual orientation, while others who identify as heterosexual might choose not to report same-sex or both-sex sexual activity. Nonetheless, given that STI kits within the OPSS are provided on the basis of self-declared information, our study demonstrates that a substantial proportion of NG infections would be missed where testing policy supports genital only testing in heterosexuals.
While NAAT is highly sensitive compared with culture,28 it cannot distinguish between viable and non-viable organisms29 and may produce false positives due to cross-reactivity with commensal Neisseria sp, such as N. meningitidis at extragenital sites.30 This risk is heightened in low-prevalence populations.31 To minimise false positives commonly associated with NAAT, the OPSS employs a dual-target confirmation approach using two distinct regions of the 16S ribosomal RNA subunit.
Conclusion
The diagnosis of isolated OPNG was significantly more common than genital diagnoses. This suggests that the oropharynx may serve as a reservoir for N. gonorrhoeae in young people. The clinical and public health significance of this warrants further investigation. If OPNG contributes to the growing epidemic of gonorrhoea, current selective testing strategies may need to be reassessed.
Data availability statement
No data are available. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
As this analysis forms part of routine public health practice in response to a specific public health concern, it does not require review by an NHS Research Ethics Committee. This work was evaluated using the NHS Health Research Authority decision tools, which determined that the project does not constitute research under NHS guidelines. This determination is consistent with the legal mandate of the Medical Officer of Health for investigation and management of notifiable diseases in Ireland.32
References
Footnotes
Handling editor Eric PF Chow
X @abbieJHarrison
Presented at Preliminary findings from this study were presented at the British Association for Sexual Health and HIV (BASHH) Annual Conference 2024 and the International Union Against Sexually Transmitted Infections (IUSTI) 2024 Conference. The abstract for the BASHH 2024 presentation is published in the International Journal of STD & AIDS.32 At IUSTI 2024, the findings were delivered during the 'Epidemiology and Surveillance' session on Thursday, 19 September 2024, Sydney, Australia. As this presentation was part of the late-breaker category, the abstract is not published.
Contributors AH: analysis protocol, analysis, manuscript writing. JH: analysis. AS, CN, DTB, FL, PB, KO'D, DI, MC, MP: input to overall protocol, review of findings and review of manuscript. RC: input to overall protocol, review of findings, manuscript writing. AH is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.